
 Gabriel
GabrielDiabetic ketoacidosis (DKA) and hyperosmolar hyperglycemic state (HHS, also known as hyperosmotic hyperglycemic nonketotic state [HHNK]) are two of the most serious acute complications of diabetes. DKA is characterized by ketoacidosis and hyperglycemia, while HHS usually has more severe hyperglycemia but no ketoacidosis. Each represents an extreme in the spectrum of hyperglycemia.
Precipitating factors
A precipitating event can usually be identified in patients with DKA or HHS. The most common are infection (eg, pneumonia, urinary tract infection, COVID-19) and discontinuation of, or inadequate, insulin therapy.
Clinical presentation
Neurologic symptoms, which may include focal findings, are more often seen in HHS and primarily occur when the effective plasma osmolality (Posm) is greater than 320 to 330 mosmol/kg. The presence of stupor or coma in diabetic patients with an effective Posm below 320 mosmol/kg demands immediate consideration of other causes of the mental status change. Abdominal pain is common in DKA, but not in HHS, and requires evaluation if it does not resolve with treatment of the acidosis. Infection can occur without fever.
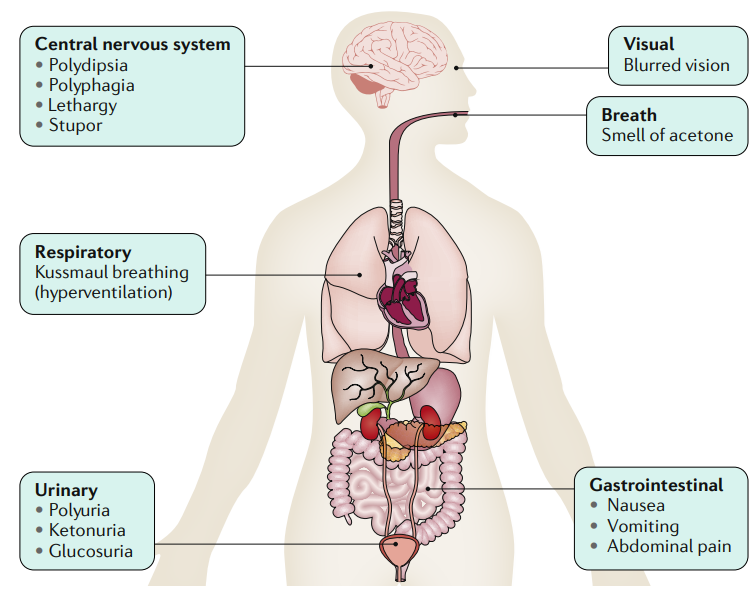
The osmotic diuresis induced by hyperglycaemia and ketonuria causes circulatory volume depletion; this, in turn, can cause the lethargy, stupor and coma. The metabolic acidosis stimulates respiratory compensation with the classic hyperventilation (‘air hunger’) that is Kussmaul breathing — the volatile ketones can be smelt on the breath. Changes in visual acuity, thought to be due to changes in water content in the eyeball or the lens, are also observed. Patients with diabetic ketoacidosis (DKA) also experience abdominal pain, nausea and vomiting that resolve with treatment.
Diagnostic evaluation
The initial evaluation of patients with hyperglycemic crises should include assessment of cardiorespiratory status, volume status, and mental status.
The initial laboratory evaluation of a patient with suspected DKA or HHS should include determination of serum glucose; electrolytes (with calculation of the anion gap), blood urea nitrogen (BUN), and plasma creatinine; complete blood count (CBC) with differential; urinalysis and urine ketones by dipstick; Posm; serum ketones; arterial blood gas (if the serum bicarbonate is substantially reduced or hypoxia is suspected); and electrocardiogram.
Laboratory findings
Diabetic ketoacidosis (DKA) and hyperosmolar hyperglycemic state (HHS) primarily differ according to the presence of ketoacidosis and the degree of hyperglycemia.
Serum ketones
Three ketone bodies are produced in DKA: one ketoacid (acetoacetic acid), one hydroxyacid (beta-hydroxybutyric acid), and one neutral ketone (acetone). Urine ketone bodies are detected by a dipstick with nitroprusside tests, while serum ketones can be detected by direct assay of beta-hydroxybutyrate levels or with a nitroprusside test. Direct assay of beta-hydroxybutyrate levels is preferred.
Anion gap metabolic acidosis
Patients with DKA usually present with a serum anion gap greater than 20 mEq/L. However, the increase in anion gap is variable, being determined by several factors: the rate and duration of ketoacid production, the rate of metabolism of the ketoacids and their loss in the urine, and the volume of distribution of the ketoacid anions.
Serum sodium
Most patients with DKA and HHS are mildly hyponatremic, but patients who have a marked osmotic diuresis may have a normal or even elevated serum sodium (Na) concentration. The serum Na concentration in DKA and HHS reflects the balance between the dilutional effect of water moving out of cells in response to the hyperglycemia-induced increase in serum osmolality and the increase in electrolyte-free water excretion due to the glucosuria-induced osmotic diuresis.
Potassium deficit
Patients with DKA or HHS have a potassium deficit that averages 300 to 600 mEq. Despite this deficit, the serum potassium concentration is often elevated at presentation, as both insulin deficiency and hyperosmolality result in potassium movement out of the cells into the extracellular fluid (ECF). Insulin therapy lowers the potassium concentration and may cause severe hypokalemia, particularly in patients with a normal or low serum potassium concentration at presentation. Thus, careful monitoring and timely administration of potassium supplementation are essential.
Amylase and lipase
Serum amylase and lipase levels are elevated in 15 to 25 percent of patients with DKA and, in most cases, do not reflect acute pancreatitis. The diagnosis of pancreatitis should be based upon clinical findings and confirmed by imaging.
Diagnostic criteria
DKA
DKA is diagnosed when the triad of hyperglycemia, anion gap metabolic acidosis, and ketonemia is present. Metabolic acidosis is often the major finding. The serum glucose concentration is usually less than 800 mg/dL (44 mmol/L) and generally between 350 to 500 mg/dL.
HHS
In HHS, there is little or no ketoacid accumulation, the serum glucose concentration may exceed 1000 mg/dL (56 mmol/L), the effective Posm is >320 mosmol/kg, and neurologic abnormalities are frequently present (including coma in 25 to 50 percent of cases).
Differential diagnosis
Ketoacidosis may also be caused by alcohol abuse or fasting. Other causes of an anion gap acidosis include lactic acidosis, ingestion of drugs such as aspirin, methanol, and ethylene glycol, and advanced chronic kidney disease
 Cargando…
Cargando…
Cargando…
Cargando…
Cargando…
Cargando…
Cargando…
Cargando…



